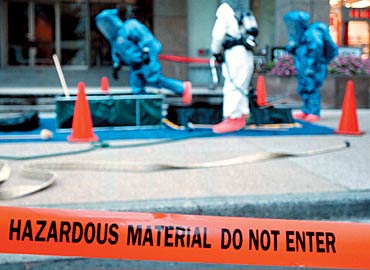
Anthrax Vaccine for Emergency Responders: Petition in support of the language of H.R. 1300 and S. 1915 to allow emergency responder access to nearly expiring anthrax vaccine from the Strategic National Stockpile
Photo: D Mackinnon/Getty Images
Act NOW! Sign the PETITION!
Please join the 465 other citizens in signing this petition in support of the language of H.R. 1300 and S. 1915 by adding your name, town, and zip code to the form below. These bills allow emergency providers access to stockpiled anthrax vaccines. Once enough names have been added to the petition, we will send the list of names to the U.S. Senate and to the President of the United States to ensure your voice is heard in support of the safety for all of America’s emergency first responders.
(*NOTE: We believe in privacy and will not sell or give your name or email address to anyone and is only used to help ensure against factitious signatories to the petition. The email addresses will be stripped from the petition prior to mailing.)
Background
Federal preparedness leaders are not acknowledging the potential of antibiotic-resistant anthrax and are not fully disclosing that antibiotics and personal protective equipment (PPE) may fail to protect first responders and volunteers as they perform their duties. Moreover, these federal stewards are unwilling or unable to share the anthrax vaccine and the protection it bestows. Instead, each year millions of federal, stockpiled doses of the anthrax vaccine expire, unused.
Project EQUIPP is a grassroots advocacy campaign formed in 2007 on behalf of local emergency responders and civilian preparedness volunteers and helped to develop a consensus paper calling for pre-exposure vaccination against anthrax for emergency responders. Shortly thereafter, the CDC Advisory Committee on Immunization Practices (ACIP) convened a working group that would ultimately revise the CDC guidance on the use of the anthrax vaccine. These CDC Recommendations were voted upon and approved in 2009. In its Notice to Readers published in MMWR in July 2010, the CDC states its support of voluntary, pre-exposure immunization with the anthrax vaccine for “persons involved in emergency response activities including but not limited to, police departments, fire departments, hazardous material units, government responders, and the National Guard.”
Bacillus anthracis bacteria, which causes the disease anthrax, is depicted here in a photograph that uses the Gram stain. Credit: Public Health Image Library (PHIL), Center for Disease Control and Prevention
H.R. 1300: The First Responder Anthrax Preparedness Act
Subsequently, on July 29, 2015, the U.S. House of Representatives unanimously passed H.R. 1300, “The First Responder Anthrax Preparedness Act,” sponsored by Congressman Peter King (R-NY). According to the nonpartisan Congressional Research Service, “The First Responder Anthrax Preparedness Act”…
… amends the Homeland Security Act of 2002 to direct the Department of Homeland Security (DHS), in coordination with the Department of Health and Human Services (HHS), for the purpose of domestic preparedness for and collective response to terrorism, to:
establish a program to provide surplus anthrax vaccines nearing the end of their labeled dates of use from the strategic national stockpile for administration to emergency response providers who are at high risk of exposure to anthrax and who voluntarily consent to such administration,
distribute disclosures regarding associated benefits and risks to end users, and
conduct outreach to educate emergency response providers about the program.
Requires DHS to:
support homeland security-focused risk analysis and assessments of the threats posed by anthrax from an act of terror;
leverage homeland security intelligence capabilities and structures to enhance prevention, protection, response, and recovery efforts with respect to an anthrax terror attack; and
share information and provide tailored analytical support on threats posed by anthrax to state, local, and tribal authorities, as well as other national biosecurity and biodefense stakeholders.
Directs DHS, in coordination with HHS, to carry out a 24-month pilot program to provide anthrax vaccines to emergency response providers.
Requires DHS to:
establish a communication platform and education and training modules for such program,
conduct economic analysis of such program,
create a logistical platform for the anthrax vaccine request process,
select providers based in at least two states to participate,
provide to each participating provider disclosures and educational materials regarding the benefits and risks of any vaccine provided and of exposure to anthrax, and
submit annual reports on pilot program results and recommendations to improve pilot program participation.
Requires the report to include a plan for continuation of the DHS program to provide vaccines to emergency response providers.
Photo: AR15.com
S. 1915: The First Responder Anthrax Preparedness Act
The Senate version of “The First Responder Anthrax Preparedness Act,” S. 1915, was introduced on August 3, 2015, by Sen. Kelly Ayotte (R-NH) and has been referred to the Committee on Homeland Security and Governmental Affairs where it sits today.
H.R. 1300 would direct the Department of Homeland Security (DHS), in consultation with the Department of Health and Human Services (HHS), to provide anthrax vaccines from the Strategic National Stockpile to first responders who volunteer to receive them. Under the bill, DHS would establish a tracking system for the vaccine and would provide educational outreach for the program. The bill would direct DHS, in coordination with HHS, to establish a pilot program in at least two states to begin providing the vaccine.
Based on information provided by DHS and HHS, CBO estimates that implementing H.R. 1300 would cost about $4 million over the 2016-2020 period, assuming appropriation of the necessary amounts. Enacting H.R. 1300 would not affect direct spending or revenues; therefore, pay-as-you-go procedures do not apply.
H.R. 1300 contains no intergovernmental or private-sector mandates as defined in the Unfunded Mandates Reform Act and would not affect the budgets of state, local, or tribal governments.
Act NOW! Sign the PETITION!
Please click here to sign this petition in support of the language of H.R. 1300 and S. 1915 to ensure your voice is heard in support of the safety for all of America’s emergency first responders.
Living in northeastern Connecticut, I find myself equidistant from two area hospitals. As a health care provider and consumer, I feel that it is important to choose the professionals who will provide my care based on fact. Websites created by the Joint Commission (2011) and the U.S. Department of Health and Human Services (HHS; 2011) prove to be a helpful repository of information regarding the safety and quality of care delivered by hospitals and practitioners across the country.
Using these two websites, I will compare the three closest hospitals to my zip code: 1) Day Kimball Hospital (10.3 mi), 2) Harrington Memorial Hospital (10.0 mi), and 3) Windham Community Memorial Hospital (21.7 mi). The mean distance from my home to these hospitals is 15.85 mi. with all three being acceptable by me in distance and time in the case of an emergency. Day Kimball Hospital (DKH; 2011) is a 104-bed acute care facility located in Putnam, Connecticut. Harrington Memorial Hospital (HMH; 2009) is a 114-bed acute care facility located in Southbridge, Massachusetts. Windham Community Memorial Hospital (WCMH; n.d.) is a 130-bed acute care facility located in Windham, Connecticut.
General process of care measures account for best practices in medicine and health care. The Surgical Care Improvement Project has set goals preventing untoward cardiac effects during certain surgical procedures along with infection control measures. According to Health Compare (HHS, 2011), cumulative scores for each hospital based on general process of care measures in the Surgical Care Improvement Project are as follows: DKH=0.954, HMH=0.901, WCMH=0.935. Another general process measure aimed at providing the standard of care of heart attack victims is the Heart Attack or Chest Pain Process of Care. The cumulative scores for these reported measures are: DKH=0.967, HMH=0.973, WCMH=0.956. Another cardiac related measure is the heart failure process of care measure. The cumulative results are: DKH=0.950, HMH=0.873, WCMH=0.893. Pneumonia process of care measures are important to gauge the appropriateness of treatments provided to stave off further development of respiratory failure and sepsis, two highly conditions with increase mortality. The cumulative scores for the pneumonia process of care measures are: DKH=0.932, HMH=0.860, WCMH=0.955. The last general process of care measure reflects the adherence to best practices in treating and managing children’s asthma; however, none of the three hospitals provided data for any of the process measures of this category.
Along with process of care measures, outcome of care measures are also important as they reflect the ability of each hospital to manage the risks of mortality and morbidity in caring for their patients. Outcome measures are based on both death and readmission of heart attack, heart failure, and pneumonia patients. For all three hospitals, DKH, HMH, and WCMH, the cumulative results for outcome of care measures were not statistically different from than the national rates in all categories. Health Compare (HHS, 2011) reports these measures as such.
One final measure that I find important in choosing a hospital is the patient satisfaction scores. Cumulative scores of the Survey of Patients’ Hospital Experience allow us to compare the three hospitals: DKH=0.695, HMH=0.701, WCMH=0.677.
In ranking each of the three hospitals, I used an average of the cumulative scores for each hospital’s measure discussed above. The final score, according to the averages of the Hospital Compare (HHS, 2011) scores, is: DKH=0.900, HMH=0.862, WCMH=0.883; therefore, my first choice of hospitals, according to the data presented in Hospital Compare is DKH with WCMH being second and HMH third. According to this data, though, each of the three hospitals appears to be equitable with the others striving in some measures and faltering in others. This is also evidenced by Quality Check (The Joint Commission, 2011), which shows a graphic representation of the same overall data, National Quality Improvement Goals and the Surgical Care Improvement Project, used by HHS (2011). Quality Check (The Joint Commission, 2011) compares quality data with the target ranges of other hospitals.
According to Quality Check (The Joint Commission, 2011), DKH met all the target goals while exceeding the goals set for infection prevention. HMH failed to meet the pneumonia care goal, but met all other goals. HMH did not exceed any of the goals. WCMH failed to meet the heart failure care goal, but met all other goals. WCMH did not exceed any of the goals.
In considering the data from Hospital Compare (HHS, 2011) and Quality Check (The Joint Commission, 2011), it is clear that this data can be used by consumers to make more informed decisions regarding their health care. Though the methods in this paper might be questionable and simple, consumers may disregard some measures while favoring others, depending on their perception of what measures are important in judging the provision of the care that they might receive. Additionally, the data used for the comparisons, many times, accounted for a small patient population; however, each hospital serves comparable communities with comparable levels of service. This may be a consideration when performing scientific statistical analyses, but that would be beyond the scope of this paper.
The provision of health care must be ethical, just, and equitable. Allowing consumers access to data regarding the performance of hospitals in their area can provide additional insight to patients when choosing their health care provider.
References
Day Kimball Hospital. (2011). Sevices and locations: Day Kimball Hospital. Retrieved from http://www.daykimball.org/services-and-locations/day-kimball-hospital/
Harrington Memorial Hospital. (2009). About us: Harrington at a glance. Retrieved from http://www.harringtonhospital.org/about_us/harrington_at_a_glance
The Joint Commission. (2011). Quality check. Retrieved from http://www.qualitycheck.org/ consumer/searchQCR.aspx
U.S. Department of Health and Human Services. (2011). Hospital compare. Retrieved from http://www.hospitalcompare.hhs.gov/
Windham Community Memorial Hospital. (n.d.). CEO’s message. Retrieved from http://www.windhamhospital.org/wh.nsf/View/CEOsMessage
Within the next 30 years, I foresee a significant public health risk of viral pandemic, a concern outlined in the recently published CISIS commission report (Fallon & Gayle, 2010). According to many, the next significant pandemic to be a global threat will occur anytime between now and 70 years (Gostin, 2004; Monto, Comanor, Shay, & Thompson, 2006; Ravilious, 2005; Smil, 2008; Tapper, 2006; Taubenberger, Morens, & Fauci, 2007). Although many scientists have their focus on influenza as the most probable for pandemic exposure, other novel virii, such as SARS, HIV, et al., have the facets to make them just as potentially significant (Gostin, 2004; Smil, 2008; Tapper, 2006). Regardless of the particular pathogen, history has shown pandemics to create and environment of negative net effects to humanity. According to Billings (1997) and Ravilious (2005), the Spanish influenza pandemic of 1918, caused by a mutated avian flu strain, claimed between 20-million and 40-million lives in a single year (Monto et al., 2006; Taubenberger et al., 2007). Spreading quickly along major international trade routes, the Spanish flu infected many servicemen returning from duty at the end of World War I. As these infected servicemen returned and celebrated the armistice in crowds of people, a severe strain on the public health system in the United States was unknowingly developing. Considering the hypervirilence and increased mortality (2.5%, compared to the typical 0.1%) caused by the 1918 Spaish flu, the world’s economy was in turmoil (Billings, 1997). As most of the American workforce was recently embroiled in overseas combat duty, upon their return they must now face the possibility of infection, an inability to work, and possible death.
Monto et al. (2006) outline a useful model of surveillance techniques that would not only be useful in detecting and improving response to influenza outbreaks, but it would certainly help to detect any new significant diseases that could be a public health risk and threaten a population or society. Additionally, Taubenberger et al. (2007) focuses on learning the biology of the influenza virus to predict the possibility of outbreak and, thus, pandemic potential. Coupling these two approaches makes sense to both identify potential pathogens and use surveillance techniques to track and direct responses to mitigate actual outbreaks as they occur. These efforts, however, should be directed by an organization that values independant operation, impartiality, neutrality, and universality, just a few of the principles of the Red Cross and Red Crescent movements (International Federation of Red Cross and Red Crescent Societies, 2010). Adoption of these principles will allow valuable health information to flow freely to other entities positioned to respond appropriately without regard to local politics, ensuring a just and equitable solution to help to mitigate the potential for great harm.
References
Billings, M. (1997/2005). The influenza pandemic of 1918. Retrieved from http://virus.stanford.edu/uda/
Fallon, W. J. & Gayle, H. D. (2010). Report of the CISIS commission on smart global health policy: A healthier, safer and more prosperous world. Washington, DC: Center for Strategic & International Studies.
Gostin, L. O. (2004). Pandemic influenza: Public health preparedness for the next global health emergency. The Journal of Law, Medicine & Ethics, 32(4), 565-573. doi:10.1111/j.1748-720X.2004.tb01962.x
International Federation of Red Cross and Red Crescent Societies. (2010, July). Haiti: From sustaining lives to sustainable solutions – the challenge of sanitation. Geneva, Switzerland: Author.
Monto, A. S., Comanor, L., Shay, D. K., & Thompson, W. W. (2006). Epidemiology of pandemic influenza: use of surveillance and modeling for pandemic preparedness. Journal of Infectious Diseases, 194(Suppl. 2), S92-S97. doi:10.1086/507559
Ravilious, K. (2005, April 14). What a way to go. The Guardian. Retrieved from http://www.guardian.co.uk/science/2005/apr/14/research.science2
Smil, V. (2008). Global catastrophes and trends: the next fifty years. Cambridge, MA: The MIT Press.
Tapper, M. L. (2006). Emerging viral diseases and infectious disease risks. Haemophilia, 12(Suppl. 1), 3–7. doi:10.1111/j.1365-2516.2006.01194.x
Taubenberger, J. K., Morens, D. M., & Fauci, A. S. (2007). The next influenza pandemic: Can it be predicted? Journal of the American Medical Association, 297(18), 2025–2027. doi:10.1001/jama.297.18.2025.
According to Hansson (2005), cardiovascular disease is fast becoming the number one killer in the world among in developing countries and the Western world, due mainly to the correlation of increased rates of obesity and diabetes (Haffner, Lehto, Rönnemaa, Pyörälä, & Laakso, 1998; Miller, 2011; Willer et al., 2008). The goal of eradicating heart disease by the end of the twentieth century has been missed as cardiovascular disease is still responsible for 38% of deaths in North America. There has been much research over the last three decades regarding correlations between cardiovascular disease, obesity, and diabetes. Miller et al. (2011) identifies, based on the current literature, a number of metabolic syndromes in which elevated triglyceride levels are responsible for significantly increasing the risk of cardiovascular disease and the risk of death from a cardiac event.
Risk factors for cardiovascular disease, including smoking, hypercholesterolemia, and diabetes, which have positive predictive value for CVD, include a positive family history, hypertension, male gender, and age (Haffner, Lehto, Rönnemaa, Pyörälä, & Laakso, 1998; Hansson, 2005; Koliaki, 2011).
Demographically, according to NHANES 1999-2008 (as cited in Miller, 2011), Mexican American men (50 to 59 years old, 58.8%) are at the greatest risk with the highest prevalence of elevated triglyceride levels ( 150 mg/dL) followed by (in order of decreasing prevalence) Mexican American women ( 70 years old, 50.5%), non-Hispanic White men (60 to 69 years old, 43.6%), non-Hispanic White women (60 to 69 years old, 42.2%), non-Hispanic Black men (40 to 49 years old, 30.4%), and non-Hispanic Black women (60 to 69 years old, 25.3%).
Haffner et al. (1998) describe the importance of lowering cholesterol levels in those with diabetes mellitus type II as they both contribute to increases in mortality and morbidity from cardiovascular disease; therefore, efforts should be focused on identifying risks to heart health starting at age 30 with concomitant risk factors of diabetes or dyslipidemia, or any combination of two or more identified risk factors. More specific screening should begin at age 40 with Mexican American males and all other demographics suffering from any one of the secondary risk-factors, and at age 50 with all other ethnic demographics, regardless of the presence of risk-factors.
Specific screening for the at-risk population should include diagnostic percutaneous transthoracic coronary angiography (PTCA) and angioplasty, if needed. PTCA is a method of introducing a catheter through an artery to the coronary arteries of the heart, guided by radiology, to diagnose specific narrowing of these vessels, at which time a repair (angioplasty) can proceed immediately. PTCA, according to Koliaki et al. (2011), is the gold standard of diagnosing the presence and degree of atherosclerotic CVD. Currently, the standard for initiating PTCA requires a more acute presentation, typically complaints of chest pain or some other cardiac related illness. However, the proven safety and efficacy of PTCA may allow it to be used more as a screening tool as well as a primary coronary intervention in acute cases.
Utilizing the diffusions of innovations model of behavior change, public health entities can provide specific information to encourage interventional cardiologists to employ this technique as a focused CVD screening tool for at-risk populations (“Culture and health,” 2012). Adoption, however, is conditional on remuneration; therefore, a public health task force at the national level should investigate the potential for spending versus savings, and if significant, should disseminate the information to third-party payors (heath insurance providers, etc.) to ensure coverage when required. Additionally, grassroots efforts should be two-pronged, focusing on both the affected communities and the physicians most likely to contact the at-risk community. For the at-risk community, using mass-media, the message should simply be to discuss your risk with your physician, stop smoking, eat healthy, and exercise. The message, itself, needs to be conveyed in an effective manner, however. For the physicians, using mass-mailing and professional development campaigns, the message needs to more complex outlining risk versus reward, cost-effectiveness, and the potential for impacting a growing trend of heart-related death and disability. The American Heart Association has a proven track record of effective mass-media campaigns as well as professional development programs. So long as PTCA can be considered as an effective and cost-saving screening tool, the American Heart Association should certainly be involved in sending the message out.
Like with the proliferation of television advertisement of pharmaceuticals, using diffusions of innovations, we can get the heart-healthy message to the communities that would most benefit and the providers who can facilitate appropriate and novel screening and treatment techniques. We have already failed to eradicate CVD by the turn of the century, but if we think outside the box and develop novel approaches to consider, we may still have a chance at effectively lowering the incidence and prevalence of CVD in the years to come.
References
Culture and health. (2012). Public health and global essentials (Custom ed.; pp. 213-226). Sudbury, MA: Jones & Bartlett.
Haffner, S. M., Lehto, S., Rönnemaa, T., Pyörälä, K., & Laakso, M. (1998). Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. New England Journal of Medicine, 339(4), 229-234. doi:10.1056/NEJM199807233390404
Hansson, G. K. (2005). Inflammation, atherosclerosis, and coronary artery disease. New England Journal of Medicine, 352(16), 1685-1695. doi:10.1056/NEJMra043430
Koliaki, C., Sanidas, E., Dalianis, N., Panagiotakos, D., Papadopoulos, D., Votteas, V., & Katsilambros, N. (2011). Relationship between established cardiovascular risk factors and specific coronary angiographic findings in a large cohort of Greek catheterized patients. Angiology, 62(1), 74-80. doi:10.1177/0003319710370960
Miller, M., Stone, N. J., Ballantyne, C., Bittner, V., Criqui, M. H., Henry N. Ginsberg, H. N., … Council on the Kidney in Cardiovascular Disease (2011). Triglycerides and cardiovascular disease: A scientific statement from the American Heart Association. Circulation, 123(20), 2292-2333. doi:10.1161/CIR.0b013e3182160726
Willer, C. J., Sanna, S., Jackson, A. U., Scuteri, A., Bonnycastle, L. L., Clarke, R., … Abecasis, G. R. (2008). Newly identified loci that influence lipid concentrations and risk of coronary artery disease. Nature, 40(2), 161-169. doi:10.1038/ng.76
Appendix
P.E.R.I. Problem Identification
The health problem I have identified is cardiovascular disease (CVD). According to Hansson (2005), CVD was expected to be significantly reduced or eliminated by the turn of the century; however, cardiovascular disease remains one of the leading cause of death globally with a rise in obesity and diabetes incidence (Willer et al., 2008). The two primary factors contributing to CVD are thought to be hypercholesterolemia, or high cholesterol levels in the blood, and hypertension, or high blood pressure, and although Koliaki et al. (2011) shows no predictive value between obesity and CVD, there remains a strong correlation between obesity and diabetes (Haffner, Lehto, Rönnemaa, Pyörälä, & Laakso, 1998; Hansson, 2005). A better look at the emerging literature might provide insight as to why attempts to control cholesterol and blood pressure have largely failed to eradicate CVD.
Koliaki et al. (2011) contend that smoking, hypercholesterolemia, and diabetes have positive predictive value for CVD while a positive family history, hypertension, male gender, and age, though predictive, are significantly less specific. Considering the causative risk factors and admitting the difficulty in changing age, family history, and gender, altering smoking status, cholesterol levels, and severity of diabetes and blood pressure have all been shown to decrease the risk of CVD. However, like genetic factors such as family history and gender, researchers are finding difficulty in controlling cholesterol levels effectively in many patients, especially those with concommitant diabetes mellitus (Haffner et al., 1998; Willer, 2008). However, statin-type cholesterol-lowering medications appear to have other protective effects than merely lowering cholesterol (Hansson, 2005).
In order to combat the growing concern of cardiovascular disease and, ultimately, the increasing mortality from the same, the American Heart Association (AHA) has published a scientific statement paper regarding the latest literature and research (Miller et al., 2011). AHA has taken the lead in cardiovascular health and strives to promote best practices based on the available evidence. By promoting AHA’s position using mass-mailing campaigns to physicians practicing in primary care, emergency, cardiology, and endocrinology, we can be assured that the right message is being disseminated rapidly to those most inclined to intervene. As more physicans in the identified roles adopt the latest evidence-based practice, more at-risk patients can be screened for CVD and the contributing factors. As screening paradigms become more focused, more of the at-risk population will be identified sooner which will allow for earlier intervention decreasing overall mortality and morbidity from CVD.
P
cardiovascular disease
E
Causes: DM, type II; dyslipidemia (hypercholesterolemia); smoking; diet; exercise; gender; age Burden: increasing mortality and morbidity globally
R
Diabetes mellitus screening and control, HTN screening and control, statin-type medication prescription, PTCA screening recommendations, smoking cessation
I
AHA position, public health mailing campaign, cadre of physician groups
When considering leadership in health care, I think first of how that leadership has affected health care in particular. Being a leader in health care does not guarantee great impact; however, an effective leader can have great impact over a large scope. This is how I framed my search to find two leaders in health care to highlight in this paper.
The first leader of health care that I will discuss is Clara Barton. According to Chambers (2002), Barton, independent to a fault, has been described as having a persuasive power about her. A fairly timid girl, Barton had self-image problems growing up that were at times debilitating; however, it seemed that as long as her interest was in helping others Barton performed selflessly, with heroism and bravado usually reserved for men during the time. Barton, a school teacher, found herself in the middle of the Civil War caring and tending to the soldiers on the battlefield. Dubbed the angel of the battlefield, Barton would not cease in caring for the soldiers even under enemy fire.
Barton, according to Chambers (2002) was not a very effective manager, but she could convince anyone to do anything that she needed to get done, it was said. Barton presents with a leadership style that is transformational (Robbins & Judge, 2010). She sees a need and immediately works to fill the void, inspiring others to do the same. Barton was ultimately responsible for founding the American Red Cross, a neutral organization that today responds to over 67, 000 disasters per year providing medical supplies, food, and housing in order to promote health equity even during wartime. Barton was a socialized charismatic leader, and her accomplishments are truly inspirational (Robbins & Judge, 2010).
The second leader of health care, more so in death than in life, that I chose to discuss is Johns Hopkins. Most people are familiar with Johns Hopkins Hospital and Johns Hopkins University, but it might be surprising to know that these namesakes were only made possible by the posthumous gift of $7-million from Hopkins’s estate (Herringshaw, 1901; “Johns Hopkins,” 1891). Hopkins started life from an affluent family, but a choice to free the family’s slaves forced Hopkins out of his formal education to help on the family tobacco farm. Since leaving the family farm, it seemed, by all accounts, that Hopkins had an innate ability for business (“Johns Hopkins,” 1891). Hopkins became very successful in business early in his lifetime, and he always tried to return his good fortune to the community. This innate ability for business, along with his unwavering business ethics, would seem to make Hopkins a likable and well-respected leader, possibly invoking a sense that he was born with these traits (Borgatta, Bales, & Couch, 1954; Cawthon, 1996; Robbins & Judge, 2010). It was in the spirit of community leader that Hopkins fulfilled his final philanthropy by funding an orphanage, a university, colleges, and a hospital that to this day is world-renowned. Johns Hopkins was an authentic leader (Robbins & Judge, 2010).
Whether a leader is naturally born with certain traits or learns behaviors from their environment, what matters most is that they be prepared to lead when the time comes. Without the onus of personal responsibility, no true leaders can exist.
References
Borgatta, E. F., Bales, R. F., & Couch, A. S. (1954). Some findings relevent to the great man theory of leadership. American Sociological Review, 19(6), 755-759. doi:10.2307/2087923
Cawthon, D. L. (1996). Leadership: the great man theory revisited. Business Horizons, 39(3), 1-4. doi:10.1016/S0007-6813(96)90001-4
Chambers, L. (2002). Fearless under fire. Biography, 6(4), 64-67, 96-97.
Herringshaw, T. W. (Ed.). (1901). Johns Hopkins. Herringshaw’s encyclopedia of American biography of the nineteenth century. Retrieved from http://books.google.com/
Johns Hopkins. (1891). The national cyclopaedia of American biography (Vol. 5). Retrieved from http://books.google.com/
Robbins, S. P. & Judge, T. A. (2010). Leadership. Essentials of Organizational Behavior (pp. 159-180). Upper Saddle River, NJ: Pearson Prentice Hall.
When attempting to solve many of the issues relevant to public health, it is essential to understand the factors that contribute to disparities across various ethnic, racial, cultural and socioeconomic boundaries (Satcher & Higginbotham, 2008). In northeastern Connecticut, however, health disparities are primarily related to the socioeconomic strata, as much of the population is Caucasian and there are identifiable health disparities within this group (U.S. Census Bureau, 2002, 2008; U.S. Department of Health and Human Services, 2009). The disparity that I will focus on in this paper is mental illness.
According to Adler and Rehkopf (2008), unjust social disparity leads to greater health disparity, but what is unjust about social disparity? Adler and Rehkopf continue to describe efforts of researchers to evaluate how socioeconomic status, both, in conjunction with and independent of race or ethnicity, contribute to health disparities. There exists a significant difference in the manner in which different cultures approach mental health needs (Hatzenbuehler, Keyes, Narrow, Grant, & Hasin, 2008). Whites, who are more prone to suffering mental health issues, according to McGuire and Miranda (2008), preferring to seek professional care while Blacks are more likely to opt for self-directed care. Though Wang, Burglund, and Kessler (2001) tell of mental health treatment disparities between Whites and Blacks, in their study, 14 times more Whites responded than Blacks which may suggest that Whites are more apt to discuss mental health issues and Blacks might not unless they are motivated by extrinsic factors, such as poor care or the impression thereof. As long as Blacks are not prevented or discouraged from seeking care, there is no injustice in choosing self-care; however, it may not be the most effective option. Cultural awareness on the part of health care providers who may have an opportunity to provide health education to Blacks may alone increase the utilization of mental health services among the Black demographic.
More importantly, mental illness often exists in the presence of poverty and the lack of education. Much of the literature, such as Schwartz and Meyer (2010), seems to make the implication that low socioeconomic status is a causative risk-factor for mental illness, yet the literature also makes the distinction that one of the lowest groups on the socioeconomic ladder, Blacks, have a lower incidence, overall, of mental illness. This may be true in some instances; however, it is more likely that mental illness may be the proximal cause for an afflicted person’s socioeconomic status, especially if the illness manifested early enough to interfere with the person’s education.
More research needs to be undertaken to identify effective programs that aim to mitigate bias of mental health conditions within the community. As mental health disorders lose their stigma, more people who suffer from mental health issues will be able to seek care comfortably and unafraid, leading to increased treatment rates and increased synthesis within the community. This synthesis alone would alleviate much of the socioeconomic burden. Additionally, we need to shift our focus and strive to fix health issues locally, not nationally or globally. The world is comprised of a network of communities of individuals. Impacting the individual is the first step to affecting positive social change. Focusing on individual health will ultimately impact community, national, and global health.
The U.S. Health care system is overtaxed in caring for people with mental illness. According to Insel (2008), we need to refocus our efforts on providing care for mental illness to reduce the enormous indirect costs estimated at $193.2-billion per year. A viable solution in addressing mental illness as a health disparity, I feel, lies in understanding the manner that mental illness causes lower socioeconomic status which, in turn, causes risk of disparate care. Programs designed to aim for situational mitigation instead of mental health recovery will be less costly, more effective and, overall, more ideal. There will still be an obvious and great need for treatment and recovery programs, but with mitigation, I posit that they will be more effective, also.
References
Adler, N. E. & Rehkopf, D. H. (2008). U.S. disparities in health: descriptions, causes, and mechanisms. Annual Review of Public Health, 29(1), 235-252. doi:10.1146/annurev.publhealth.29.020907.090852
Hatzenbuehler, M. L., Keyes, K. M., Narrow, W. E., Grant, B. F., & Hasin, D. S. (2008). Racial/ethnic disparities in service utilization for individuals with co-occurring mental health and substance use disorders in the general population. Journal of Clinical Psychology, 69(7), 1112-1121. doi:10.4088/JCP.v69n0711
Insel, T. R. (2008). Assessing the economic costs of serious mental illness. American Journal of Psychiatry, 165, 663-665. doi:10.1176/appi.ajp.2008.08030366
McGuire, T. G. & Miranda, J. (2008). New evidence regarding racial and ethnic disparities in mental health: policy implications. Health Affairs, 27(2), 393-403. doi:10.1377/hlthaff.27.2.393
Newport, F. & Mendes, E. (2009, July 22). About one in six U.S. adults are without health insurance: Highest uninsured rates among Hispanics, the young, and those with low incomes. Gallup-Heathways Well-Being Index. Retrieved from http://www.gallup.com/poll/121820/one-six-adults-without-health-insurance.aspx
Satcher, D. & Higginbotham, E. J. (2008). The public health approach to eliminating health disparities. American Journal of Public Health, 98(3), 400–403. doi:10.2105/AJPH.2007.123919
Schwartz, S. & Meyer, I. H. (2010). Mental health disparities research: The impact of within and between group analyses on tests of social stress hypotheses. Social Science and Medicine, 70, 1111-1118. doi:10.1016/j.socscimed.2009.11.032
U.S. Census Bureau. (2002). Census 2000. Retrieved from http://www.ct.gov/ecd/cwp/view.asp?a=1106&q=250616
U.S. Census Bureau. (2008). Population estimates: Annual estimates of the resident population by age, sex, race, and Hispanic origin for counties in Connecticut: April 1, 2000 to July 1, 2008 [Data]. Retrieved from http://www.census.gov/popest/counties/asrh/files/cc-est2008-alldata-09.csv
U.S. Department of Health and Human Services. (2009). Community health status indicators report. Retrieved from http://communityhealth.hhs.gov/
I currently reside in Windham County, Connecticut. Windham County is primarily rural with one community, Willimantic, comprising most of the urban demographic. Windham County is functionally divided in half (north to south) in regards to health and hospital services. Primarily, Windham Community Memorial Hospital serves the west and Day Kimball Hospital serves the east. Accordingly, the eastern and western portions of the county may not be representative of each other, yet both are represented as a singular group when considering county-based statistics. This is a shortcoming of county-based statistics. In this instance, Willimantic, in the western portion of Windham County, may negatively affect the statistics of towns like Killingly, Pomfret, and Putnam, in the eastern portion of the county, due primarily to an increase in impoverished populations residing in Willimantic (U.S. Census Bureau, 2002). Additionally, data is lacking for a number of measures, according to the Community Health Status Indicators Project Working Group (2009), but continuing efforts will be made to increase reporting over time.
According to the U.S. Census Bureau (2008) and the U.S. Department of Health and Human Services (2009), the population of Windham County is 117,345 and is predominantly white (94.3%) with the remaining (5.7%) divided among, in order of predominance, Hispanics, Blacks, Asians and Pacific Islanders, and American Indians. The particularly vulnerable populations identified are adults age 25 and older who do not hold a high school diploma, are unemployed, are severely disabled and unable to work, suffer major depression, or have recently used illicit drugs. The uninsured rate in Windham County is well below the 16% national average at 9.5% (Newport & Mendes, 2009; U.S. Department of Health and Human Services, 2009).
Windham County fares equal or better in most measures, at least within the margin of error; therefore, I feel that Windham County, though not exceptionally healthy, is better than most and striving to meet the national standards (U.S. Department of Health and Human Services, 2009). For example, though the incidence of cancer and subsequent death resulting remains higher than peer counties, Windham County falls well within the expected range of death measures and exceeds peer counties in homicide, stroke, suicide, and unintentional injuries. Windham County also falls below the national standardized target for both stroke and coronary heart disease deaths. Infant mortality and birth measures seem representative of peer counties. Windham County also meets or exceeds environmental standards in all cases except for two reports of E. coli infections. There were also reports of five cases of Haemophilus influenzae B, two cases of Hepatitis A, and three cases of Hepatitis B — the only unexpected cases of infectious diseases reported. Pertussis incidence was limited to 25% of expected cases.
Windham County is not exceptional, but living here gives me the sense that the focus is on preventative care rather than acute care, which might explain how the health goals are being achieved overall. The report from the U.S. Department of Health and Human Services (2009) is in agreement.
References
Community Health Status Indicators Project Working Group. (2009). Data sources, definitions, and notes for CHSI2009. Retrieved from http://communityhealth.hhs.gov/
Newport, F. & Mendes, E. (2009, July 22). About one in six U.S. adults are without health insurance: Highest uninsured rates among Hispanics, the young, and those with low incomes. Gallup-Heathways Well-Being Index. Retrieved from http://www.gallup.com/poll/121820/one-six-adults-without-health-insurance.aspx
U.S. Census Bureau. (2002). Census 2000. Retrieved from http://www.ct.gov/ecd/cwp/view.asp?a=1106&q=250616
U.S. Census Bureau. (2008). Population estimates: Annual estimates of the resident population by age, sex, race, and Hispanic origin for counties in Connecticut: April 1, 2000 to July 1, 2008 [Data]. Retrieved from http://www.census.gov/popest/counties/asrh/files/cc-est2008-alldata-09.csv
U.S. Department of Health and Human Services. (2009). Community health status indicators report. Retrieved from http://communityhealth.hhs.gov/
I have always maintained that the best thing that I have ever done for a patient was to hold their hand as they died; however, there are few scenarios that I can posit where I would ever cause the death of another, and I would never do it in my capacity as a medical professional. In the State of Connecticut, assisting a patient in their suicide is illegal (Kasprak, 2003; Saunders & Smith, 2010). Saunders and Smith (2010) describe the use of “semantic ploys” (para. 3) in arguing for physician-assisted suicide and how the court deemed the “issue rests with the legislature, not with the court” (para 4).
Two states have laws permitting physician-assisted suicide, Oregon and Washington (Death with Dignity Act, 1997; Death with Dignity Act, 2008). The other 48 states either have laws forbidding assisted suicide, such as Connecticut, rely on common law, or have no laws permitting or forbidding the practice (Kasprak, 2003). Personally, my thoughts on the matter are clearly reflected in my opening statement. More compelling, however, is a recent discussion on the discontinuation of implanted cardiac devices in patients with a desire to “refuse continued life-sustaining therapy” (Kapa, Mueller, Hayes, & Asirvatham, 2010, p. 989). Many of the respondants to this study viewed the discontinuation of pacemakers akin to physician-assisted suicide, whereas less felt the termination of cardioverter-defibrillator therapy was an ethical issue. Oddly, lawyers indicated less problems discontinuing therapy than did physicians.
There are conditions that are so intractably painful and wrought with suffering that I would not even consider thinking less of a person suffering such a malady who took their own life. Death, for many people, is a fear beyond fear, and for a person (of considerable sound mind) to choose death as a viable alternative to such suffering, I commend their bravery and choose not to judge them negatively. No physician or other health care provider should cause the death of a person directly, but acknowledging the patient’s will to die is another matter. In lieu of providing a chemical means of ending life, a physician could, in my mind, counsel a patient on the means and methods that might be viewed as more effective and humane than other means which might result in unwanted suffering. I do believe that a person has the right to choose an alternative to a surely painful and agonizing death, regardless of the presence of depression. If a person is suffering from depression because of a terminal illness that is causing physical suffering, it is hard to imagine this person will resolve the depression before succumbing to the causal disease process. In these cases, the person has the right to choose a more dignified death. For those cases where the person is incapacitated and cannot make health care decisions, I feel that any friend or family member, or a consensus of available friends and family members, should be able to make the decision to continue or discontinue life-sustaining measures. Even if the decision is wrong for the patient, most of the time the decision is for the benefit of the family and friends and lacks medical relevance aside from resource management, though there are spiritual, emotional, and moral considerations that the next of kin may face which are no less relevant.
Personally, I grant any person permission to end my life if they see me engulfed in flame or if taken on the battlefield by an enemy known for public torture. Beyond these two circumstances, I will always choose to live so long as I have my thoughts. I have heard some people intimate that they would wish to die if they were conscious but perpetually paralyzed (i.e. locked-in syndrome); however, I am not so sure that I would want to die just for lacking the ability to communicate with others. I would want to view the world, though, perhaps by television or radio. I am too curious as to what comes next for the world. As we interfere with the dying process, it does make sense that we address the morality in which we do this. It does not seem right to have brain dead patients connected to ventilators and feeding tubes forever. It’s Orwellian.
References
Death with Dignity Act of 1997, O.R.S. 127.800 et seq. (1997).
Death with Dignity Act of 2009, R.C.W. 70.245 (2008).
Kapa, S., Mueller, P. S., Hayes, D. L., & Asirvatham, S. J. (2010). Perspectives on withdrawing pacemaker and implantable cardioverter-defibrillator therapies at end of life: Results of a survey of medical and legal professionals and patients. Mayo Clinic Proceedings, 85(11), 981-990. doi:10.4065/mcp.2010.0431
Kasprak, J. (2003, July 9). Assisted suicide (OLR Research Report No. 2003-R-0515). Retrieved from http://www.cga.ct.gov/2003/olrdata/ph/rpt/2003-R-0515.htm
Saunders, W. L. & Smith, M. R. (2010, June 21). Assisted-suicide advocates fail in Connecticut. National Review Online. Retrieved from http://www.nationalreview.com
Disparities in the availability, access, and delivery of health care are a great and growing concern. Some of the factors leading to disparite health include race, socioeconomic status, and gender (Chen, Martin, & Mattews, 2006). Chen et al. describes how race and socioeconomic status are major factors in the United States, based on the Healthy People 2010 data (U.S. Department of Health and Human Services, 2000). According to the results of this study, our public health efforts seem to be misguided. As the researchers of this study indicate, “race and SES effects on child health are best understood in concert, rather than separately” (p. 705). The differences in race and socioeconomic status are a factor only to White and Black children when looking at prevalence rates for activity limitations and circulatory conditions, as illustrated by Chen et al. in Figures 1 and 2. These figures show that higher education actually has a small but negative effect on the health status of Asians and Hispanics while having a dramatically positive effect on Blacks. Additionally, in Figure 3, Chen et al. show a significant negative effect of education on incidence rates for acute respiratory conditions. There is no significant relationship for the same with regards to Whites or Blacks.
This study shows that there are certainly correlations between race, economic status, and differences in the health status of children in America, but these factors might only be relative. We need to understand if other factors can be identified as causative. In order to explain how Whites and Blacks share correlations while Asians and Hispanics share correlations, we might consider the length of time each population has been exposed to American culture. Whites and Blacks have been in America for over 300 years while Asians and Hispanics have migrated more recently. In addition, there is also evidence of attitude and preference differences for minorities towards health care, though the Institute of Medicine (2002) marginalizes this phenomena in their study.
As a health care provider and regardless of the causes of disparities in health status, it is advisable that I understand these causes so that I may better direct a patient’s care with a holistic understanding of the patient.
References
Chen, E., Martin, A. D., & Matthews, K. A. (2006). Understanding health disparities: The role of race and socioeconomic status in children’s health. American Journal of Public Health, 96, 702-708. doi:10.2105/AJPH.2004.048124
Institute of Medicine. (2002). Unequal treatment: What healthcare providers need to know about racial and ethnic disparities in health. Retrieved from http://www.nap.edu/html/unequal_treatment/reportbrief.pdf
U.S. Department of Health and Human Services. (2000). Healthy people 2010: Understanding and improving health. Washington, DC: Author.
Cultural Models of Immunization and Infectious Disease Mitigation
The members of some communities, such as Puerto Rico, do not understand the scope and severity of some infectious diseases until they become infected (Pérez-Guerra, Zielinski-Gutierrez, Vargas-Torres, & Clark, 2009). The lack of a basic understanding of illness and infection poses a roadblock to mitigating disease transmission within the community. For Pérez-Guerra et al., the perception of severity and mitigation is important as they investigate the difference in attitudes towards dengue infections because dengue cannot be controlled by vaccine and must be mitigated by community participation in mosquito abatement activities. Other infectious diseases, however, can be controlled by vaccine, but efforts to limit infection are met with ignorance or misconceptions (Lau, Griffiths, Choi, & Tsui, 2010; Leask, Sheikh-Mohammed, MacIntyre, Leask, & Wood, 2006).
Public health officials, in concert with community leaders, should seek to educate affected communities about the infectious diseases they face along with effective mitigation strategies and the importance of vaccination, if available. Coreil (2010) describes the importance of cultural models in “[gaining] a deeper understanding of the cultural context of behavior” (p. 83). If behaviors are not understood, then it will be difficult to redirect them. Reaching out to community leaders has the added effect of allowing the leaders to alter the message just enough so that it might be effectively communicated to the community.
Providing a cultural health model allows for a larger scope of audience while effectively tailoring the message so that most of the target audience will appreciate the nature of the message. Approaching health behaviors from a cultural stand-point also offers the advantage of allowing peer support to propagate messages through out the community. This might be especially true when dealing with a multitude of subcultures where the message might better be disseminated via interpersonal means. Eventually, the message will be received by many individuals who will begin to have discussions with others in the community. For communities where individuals are not likely to speak to each other regarding personal health-related matters, the cultural health model allows a general message to reach each individual.
References
Coreil, J. (Ed.). (2010). Social and behavioral foundations of public health (2nd ed.). Thousand Oaks, CA: Sage.
Lau, J. T. F., Griffiths, S., Choi, K. C., & Tsui, H. Y. (2010). Avoidance behaviors and negative psychological responses in the general population in the initial stage of the H1N1 pandemic in Hong Kong. BMC Infectious Diseases, 10(139), 1-13. doi:10.1186/1471-2334-10-139
Leask, J., Sheikh-Mohammed, M., MacIntyre, C. R., Leask, A., & Wood, N. J. (2006). Community perceptions about infectious disease risk posed by new arrivals: A qualitative study. The Medical Journal of Australia, 185(11/12), 591-593. Retrieved from http://www.mja.com.au/public/issues/185_11_041206/lea10999_fm.pdf
Pérez-Guerra, C. L., Zielinski-Gutierrez, E., Vargas-Torres, D., & Clark, G. G. (2009). Community beliefs and practices about dengue in Puerto Rico. Pan American Journal of Public Health, 25(3), 218-226. doi:10.1590/S1020-49892009000300005