Anthrax Vaccine for Emergency Responders: Petition in support of the language of H.R. 1300 and S. 1915 to allow emergency responder access to nearly expiring anthrax vaccine from the Strategic National Stockpile
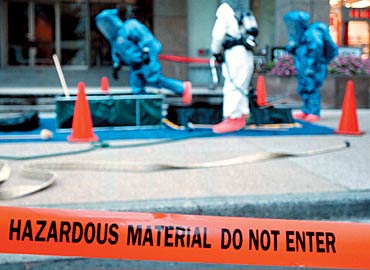
Photo: D Mackinnon/Getty Images
Act NOW! Sign the PETITION!
Please join the 465 other citizens in signing this petition in support of the language of H.R. 1300 and S. 1915 by adding your name, town, and zip code to the form below. These bills allow emergency providers access to stockpiled anthrax vaccines. Once enough names have been added to the petition, we will send the list of names to the U.S. Senate and to the President of the United States to ensure your voice is heard in support of the safety for all of America’s emergency first responders.
(*NOTE: We believe in privacy and will not sell or give your name or email address to anyone and is only used to help ensure against factitious signatories to the petition. The email addresses will be stripped from the petition prior to mailing.)
Background
Federal preparedness leaders are not acknowledging the potential of antibiotic-resistant anthrax and are not fully disclosing that antibiotics and personal protective equipment (PPE) may fail to protect first responders and volunteers as they perform their duties. Moreover, these federal stewards are unwilling or unable to share the anthrax vaccine and the protection it bestows. Instead, each year millions of federal, stockpiled doses of the anthrax vaccine expire, unused.
Project EQUIPP is a grassroots advocacy campaign formed in 2007 on behalf of local emergency responders and civilian preparedness volunteers and helped to develop a consensus paper calling for pre-exposure vaccination against anthrax for emergency responders. Shortly thereafter, the CDC Advisory Committee on Immunization Practices (ACIP) convened a working group that would ultimately revise the CDC guidance on the use of the anthrax vaccine. These CDC Recommendations were voted upon and approved in 2009. In its Notice to Readers published in MMWR in July 2010, the CDC states its support of voluntary, pre-exposure immunization with the anthrax vaccine for “persons involved in emergency response activities including but not limited to, police departments, fire departments, hazardous material units, government responders, and the National Guard.”
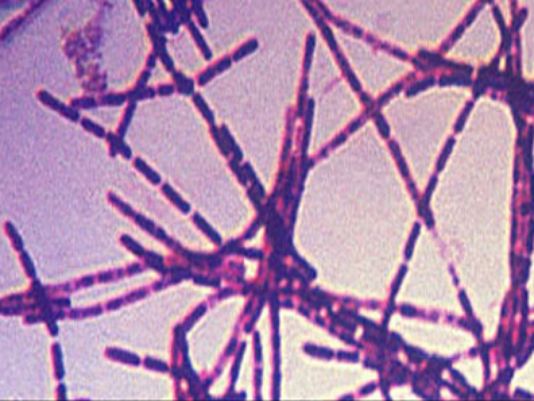
Bacillus anthracis bacteria, which causes the disease anthrax, is depicted here in a photograph that uses the Gram stain. Credit: Public Health Image Library (PHIL), Center for Disease Control and Prevention
H.R. 1300: The First Responder Anthrax Preparedness Act
Subsequently, on July 29, 2015, the U.S. House of Representatives unanimously passed H.R. 1300, “The First Responder Anthrax Preparedness Act,” sponsored by Congressman Peter King (R-NY). According to the nonpartisan Congressional Research Service, “The First Responder Anthrax Preparedness Act”…
… amends the Homeland Security Act of 2002 to direct the Department of Homeland Security (DHS), in coordination with the Department of Health and Human Services (HHS), for the purpose of domestic preparedness for and collective response to terrorism, to:
establish a program to provide surplus anthrax vaccines nearing the end of their labeled dates of use from the strategic national stockpile for administration to emergency response providers who are at high risk of exposure to anthrax and who voluntarily consent to such administration,
distribute disclosures regarding associated benefits and risks to end users, and
conduct outreach to educate emergency response providers about the program.
Requires DHS to:
support homeland security-focused risk analysis and assessments of the threats posed by anthrax from an act of terror;
leverage homeland security intelligence capabilities and structures to enhance prevention, protection, response, and recovery efforts with respect to an anthrax terror attack; and
share information and provide tailored analytical support on threats posed by anthrax to state, local, and tribal authorities, as well as other national biosecurity and biodefense stakeholders.
Directs DHS, in coordination with HHS, to carry out a 24-month pilot program to provide anthrax vaccines to emergency response providers.
Requires DHS to:
establish a communication platform and education and training modules for such program,
conduct economic analysis of such program,
create a logistical platform for the anthrax vaccine request process,
select providers based in at least two states to participate,
provide to each participating provider disclosures and educational materials regarding the benefits and risks of any vaccine provided and of exposure to anthrax, and
submit annual reports on pilot program results and recommendations to improve pilot program participation.
Requires the report to include a plan for continuation of the DHS program to provide vaccines to emergency response providers.
Photo: AR15.com
S. 1915: The First Responder Anthrax Preparedness Act
The Senate version of “The First Responder Anthrax Preparedness Act,” S. 1915, was introduced on August 3, 2015, by Sen. Kelly Ayotte (R-NH) and has been referred to the Committee on Homeland Security and Governmental Affairs where it sits today.
H.R. 1300 would direct the Department of Homeland Security (DHS), in consultation with the Department of Health and Human Services (HHS), to provide anthrax vaccines from the Strategic National Stockpile to first responders who volunteer to receive them. Under the bill, DHS would establish a tracking system for the vaccine and would provide educational outreach for the program. The bill would direct DHS, in coordination with HHS, to establish a pilot program in at least two states to begin providing the vaccine.
Based on information provided by DHS and HHS, CBO estimates that implementing H.R. 1300 would cost about $4 million over the 2016-2020 period, assuming appropriation of the necessary amounts. Enacting H.R. 1300 would not affect direct spending or revenues; therefore, pay-as-you-go procedures do not apply.
H.R. 1300 contains no intergovernmental or private-sector mandates as defined in the Unfunded Mandates Reform Act and would not affect the budgets of state, local, or tribal governments.
Act NOW! Sign the PETITION!
Please click here to sign this petition in support of the language of H.R. 1300 and S. 1915 to ensure your voice is heard in support of the safety for all of America’s emergency first responders.
Cultural Models of Immunization and Infectious Disease Mitigation
The members of some communities, such as Puerto Rico, do not understand the scope and severity of some infectious diseases until they become infected (Pérez-Guerra, Zielinski-Gutierrez, Vargas-Torres, & Clark, 2009). The lack of a basic understanding of illness and infection poses a roadblock to mitigating disease transmission within the community. For Pérez-Guerra et al., the perception of severity and mitigation is important as they investigate the difference in attitudes towards dengue infections because dengue cannot be controlled by vaccine and must be mitigated by community participation in mosquito abatement activities. Other infectious diseases, however, can be controlled by vaccine, but efforts to limit infection are met with ignorance or misconceptions (Lau, Griffiths, Choi, & Tsui, 2010; Leask, Sheikh-Mohammed, MacIntyre, Leask, & Wood, 2006).
Public health officials, in concert with community leaders, should seek to educate affected communities about the infectious diseases they face along with effective mitigation strategies and the importance of vaccination, if available. Coreil (2010) describes the importance of cultural models in “[gaining] a deeper understanding of the cultural context of behavior” (p. 83). If behaviors are not understood, then it will be difficult to redirect them. Reaching out to community leaders has the added effect of allowing the leaders to alter the message just enough so that it might be effectively communicated to the community.
Providing a cultural health model allows for a larger scope of audience while effectively tailoring the message so that most of the target audience will appreciate the nature of the message. Approaching health behaviors from a cultural stand-point also offers the advantage of allowing peer support to propagate messages through out the community. This might be especially true when dealing with a multitude of subcultures where the message might better be disseminated via interpersonal means. Eventually, the message will be received by many individuals who will begin to have discussions with others in the community. For communities where individuals are not likely to speak to each other regarding personal health-related matters, the cultural health model allows a general message to reach each individual.
References
Coreil, J. (Ed.). (2010). Social and behavioral foundations of public health (2nd ed.). Thousand Oaks, CA: Sage.
Lau, J. T. F., Griffiths, S., Choi, K. C., & Tsui, H. Y. (2010). Avoidance behaviors and negative psychological responses in the general population in the initial stage of the H1N1 pandemic in Hong Kong. BMC Infectious Diseases, 10(139), 1-13. doi:10.1186/1471-2334-10-139
Leask, J., Sheikh-Mohammed, M., MacIntyre, C. R., Leask, A., & Wood, N. J. (2006). Community perceptions about infectious disease risk posed by new arrivals: A qualitative study. The Medical Journal of Australia, 185(11/12), 591-593. Retrieved from http://www.mja.com.au/public/issues/185_11_041206/lea10999_fm.pdf
Pérez-Guerra, C. L., Zielinski-Gutierrez, E., Vargas-Torres, D., & Clark, G. G. (2009). Community beliefs and practices about dengue in Puerto Rico. Pan American Journal of Public Health, 25(3), 218-226. doi:10.1590/S1020-49892009000300005
Vaccines are very useful as preventive medicine in public health to reduce morbidity and mortality due to communicable diseases, though they are not a substitute to safe drinking water, sanitation, nutrition and environmental health in the long run.
(Madhavi et al., 2010, p. 618)
In dealing with infectious diseases, two primary methods of prevention are worthwhile: immunization and avoidance. Avoidance is nearly impossible as valence for various pathogens vary so greatly and community network structure influences (Ciccaroneet al., 2010; Salathé & Jones, 2010). Immunization, on the other hand, allows for proximal contact with a specific pathogen without the likelihood to effective transmission, or active infection. Immunization, or innoculation, is the process of introducing the immune system to potential future pathogens so that it may form lifelong antibodies that can readily attack the pathogen if infected in the future (Centers for Disease Control, 2009). Immunization is gaining stronger support in the face of a growing number of antibiotic-resistant pathogens and pathogens with a propensity for recombination under heavy environmentally selective pressures, and though antibiotic therapy is a reliable and effective secondary prevention method, it seems to be true that antibiotic therapy is becoming less effective the more we rely on it as a prophylaxis (Laxminarayan & Brown, 2001). Additionally, antibiotics are only effective in the treatment of bacterial infections and have no effect on viral infections. Antiviral medications are typically more expensive and less available.
Luckily, when speaking about infectious processes, there is little need for continuous care after the acute presentation (Ciccarone et al., 2010). The pathogen is typically eradicated from the host by means of the natural combative effects of the immune system in combination, when required, with pharmacological assistance, and there is only a small chance of the host suffering any lasting effects. Unfortunately, there are some pathogens that continue to cause harm well after the acute phase of infection. Pathogens, such as the human immunodeficiency virus, ravage the immune system making the host susceptible to a number of other opportunistic infections that can become life-threatening. Other pathogens, such as hepatitis, can damage the natural filtration system of the host’s body that other deleterious effects surface creating a chronic disease process of the organs. In these, and other, cases, tertiary prevention strategies can help to offer the host a meaningful quality of life with the presence of the disease process. Some effective tertiary methods include medications aimed at improving the function of certain organs or systems. Diet and exercise also plays a major role in tertiary prevention strategies (Stokols, 1992).
Depending on the particular pathogen, infection might not affect me as much as others. As a paramedic, I have a comfortable knowledge of infectious disease processes, and I understand that a simple regimen of antibiotic medication, along with rest and fluid intake, will cure most of the infectious bacterial diseases that I might face, albeit some drug-resistant pathogens are not so easy to manage. Additionally, I have isolation equipment at my disposal that allows me to create a barrier from these and other infectious diseases. Ciccarone et al. (2010) further describe many of the psychosocial barriers Asian and Pacific Islanders face when confronted with the early stages of some infections. “Psychosocial issues such as depression, embarrassment, and shyness were reported to have influenced time to seeking medical attention” (Ciccarone et al., 2010, p. 143). Although I accept that I may suffer one or more of these barriers, my education, along with mandatory workplace reporting requirements, empower me to seek medical care when needed.
Addressing prevention strategies, Stokols (1992) introduces a model using the social ecology of health. Though he does not categorize primary, secondary, and tertiary means, he does hint at prevention strategies being proximal or distal. Further, Stokols outlines a variety of means related directly to an understanding of environmental roles and pressures. Understanding how an individual relates to, from, and within his or her ecology allows the health practitioner to provide more focused means of prevention and education.
References
Centers for Disease Control. (2009). Parent’s Guide to Immunizations [Excerpt]. Retrieved from http://www.cdc.gov/vaccines/vac-gen/downloads/pg_how_vacc_work.pdf
Ciccarone, R. M., Kim, M., Tice, A. D., Nakata, M., Effler, P., Jernigan, D. B., … & Sinkowitz-Cochran, R. L. (2010). Prevention of community-associated methicillin-resistant staphylococcus aureus infection among Asian/Pacific Islanders: A qualitative assessment. Hawai‘i Medical Journal, 69(6), 142-144. Retrieved from http://web.ebscohost.com.ezp.waldenulibrary.org/
Laxminarayan, R. & Brown, G. M. (2001). Economics of antibiotic resistance: A theory of optimal use. Journal of Environmental Economics and Management, 42(2), 183-206. doi:10.1006/jeem.2000.1156
Madhavi, Y., Puliyel, J. M., Mathew, J. L., Raghuram, N., Phadke, A., Shiva, M., … & Banerji, D. (2010). Evidence-based national vaccine policy. Indian Journal of Medical Research, 131, 617-628. Retrieved from http://web.ebscohost.com.ezp.waldenulibrary.org/
Salathé, M. & Jones, J. H. (2010). Dynamics and control of diseases in networks with community structure. PLoS Computational Biology, 6(4), e1000736. doi:10.1371/journal.pcbi.1000736
Stokols, D. (1992). Establishing and maintaining healthy environments: Toward a social ecology of health promotion. American Psychologist, 47(1), 6-22. doi:10.1037/0003-066X.47.1.6